Many low-moderate grade well-differentiated neuroendocrine tumours (NETs) have long been identified as expressing high levels of somatostatin receptors, particularly subtypes 2 and 5.
Somatostatin analogs (SSAs) – a standard of first-line treatment in NETs – bind to somatostatin receptors and are used for managing hormonal syndromes and control of tumour growth. The long-acting SSAs octreotide long-acting release and lanreotide are commonly used in the first-line metastatic setting because of their tolerable side effect profile.
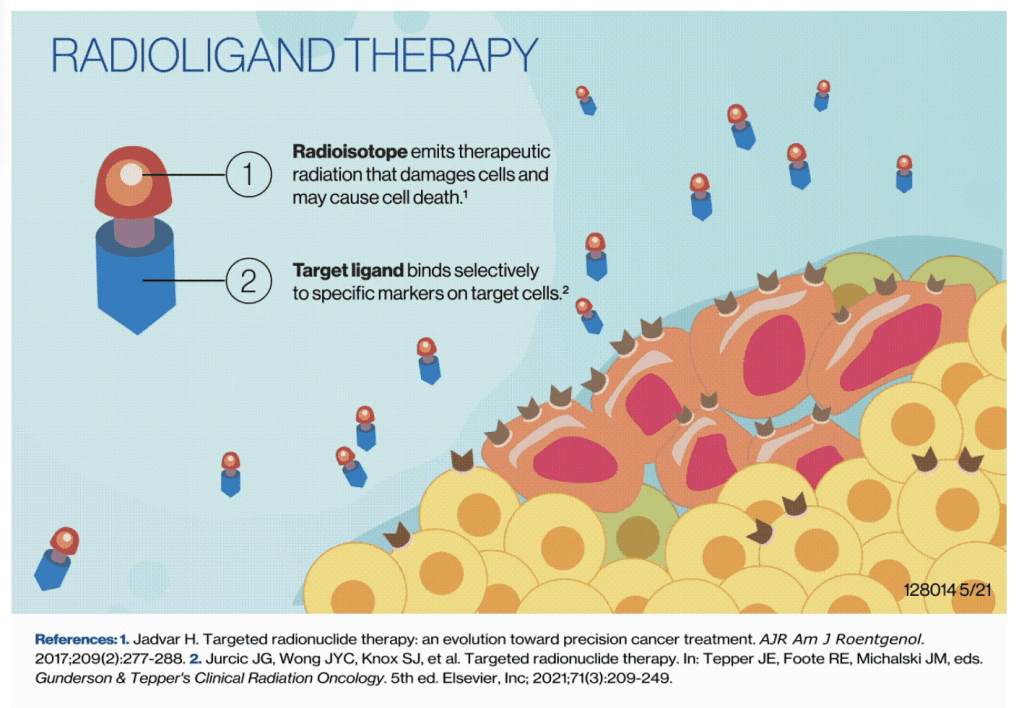
Radio-labeled SSAs are used both for imaging and for treatment of NETs:
- Gallium-68 DOTATATE (or Ga-68 DOTATATE) is a PET radio-tracer / radio-labeled SSA that is used for evaluating primary and metastatic well-differentiated neuroendocrine tumours.
- 177Lu-DOTATATE is a β-emitting radio-labeled SSA that has been proven to significantly improve progression-free survival among patients with progressive midgut NETs and is approved for treatment of Grade 1-2 metastatic gastroenteropancreatic (GEP) NETs.
–
The results from the NETTER-1 study (NCT01578239), published by Strosberg et al in 2017, established radioligand therapy (RLT) with 177Lu-Dotatate as a standard of care for those with previously treated, well-differentiated low-grade (G1-2) midgut primary neuroendocrine tumours. In the UK, this study alongside patient experience testimony was evaluated by NICE – and the treatment was approved for use within the NHS setting:
–
–
Lutetium (177Lu) oxodotreotide is recommended, within its marketing authorisation, as an option for treating unresectable or metastatic, progressive, well-differentiated (grade 1 or grade 2), somatostatin receptor-positive gastroenteropancreatic neuroendocrine tumours (NETs) in adults. NICE Technology appraisal guidance [TA539] Published: 29 August 2018
However, many experts agree that no equivalent standard of care existed for those with higher-grade GEP-NETs, providing a rationale for evaluating the radioligand in this group of patients. NETTER-2 was developed to address this unmet need:
“There is no established universal standard of care for these patients. Existing first-line treatment options for patients with high grade 2 or grade 3 well-differentiated gastroenteropancreatic neuroendocrine tumors are based on consensus guidelines with little supporting evidence.
So far, no randomized phase III studies have investigated the most appropriate treatment strategy for higher grade 2 and grade 3 gastroenteropancreatic neuroendocrine tumors, highlighting the need for more robust data to guide clinical decision-making. This study will be practice-changing,”.Simron Singh, Lead Study Author: Odette Cancer Centre, Canada
–
–
In the phase III NETTER-2 trial, (NCT03972488), a total of 226 patients newly diagnosed (within the past 6 months) with somatostatin receptor–positive high grade advanced gastroenteropancreatic neuroendocrine tumours were randomly assigned to receive either Lu-177 dotatate plus octreotide (treatment arm) or octreotide alone (control arm).
- In the treatment arm, 151 randomly assigned patients received four cycles of Lu-177 dotatate plus 30 mg of octreotide long-acting release at 8-weekly intervals.
- In the control arm, 75 randomly assigned patients received 60 mg of octreotide long-acting release every 4 weeks.
Patients had a median age of 61 years; 53.5% were male and 46.5% were female; 73.0% of patients were White, 15.0% were Asian, and 11.9% were of other races.
–
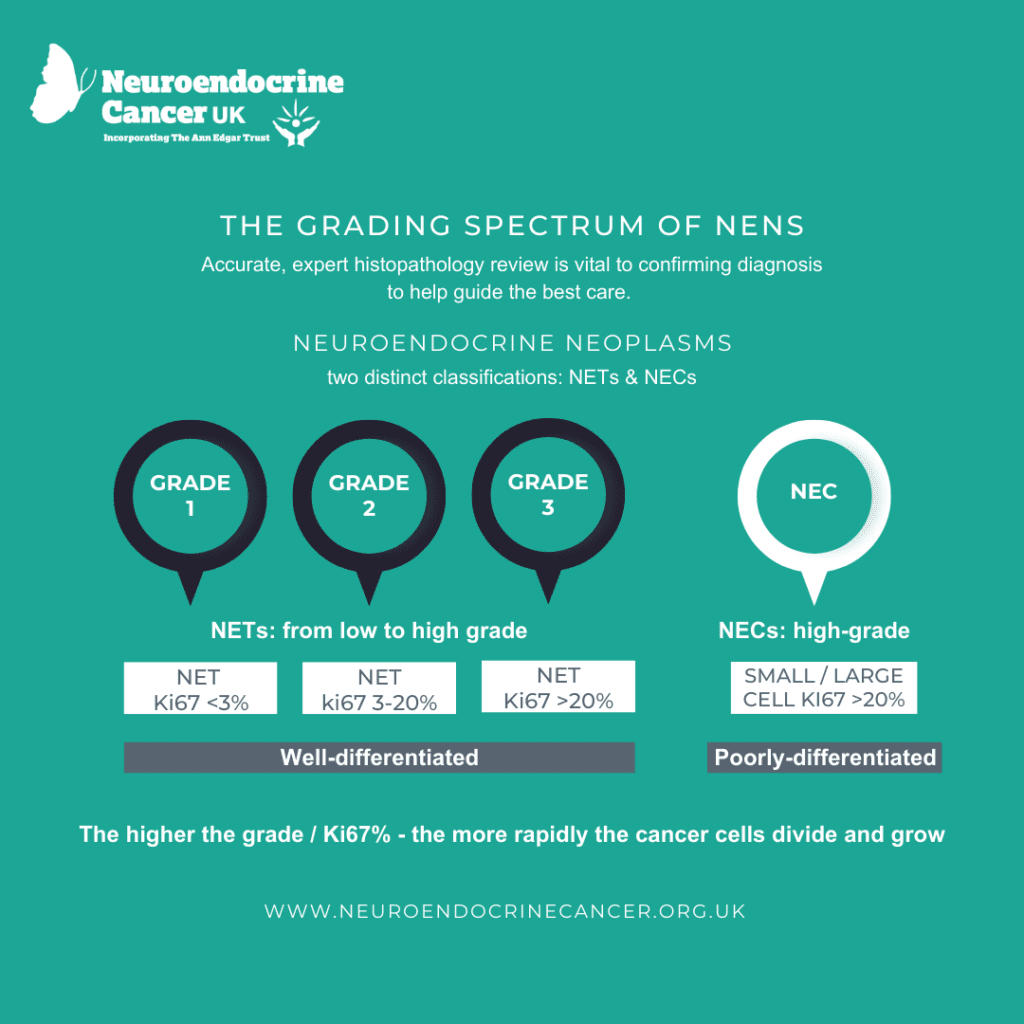
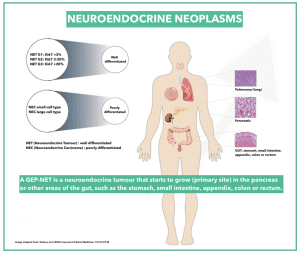 Patients were stratified by grade (grade 2 or grade 3: Ki67 10-55%) and tumour primary site (pancreas vs other location):
Patients were stratified by grade (grade 2 or grade 3: Ki67 10-55%) and tumour primary site (pancreas vs other location):
- 65% = Grade 2
- 35% = Grade 3
- 54.4% = primary pancreas,
- 29.2% = primary small bowel
.
The primary endpoint of the trial was progression-free survival; the secondary endpoint was objective response rate.
At this month’s ASCO Gastrointestinal Cancers Symposium (GiCS), Dr Singh reported the results:
“NETTER-2 met its primary endpoint, reducing the risk of progression or death by 72%. The response rate observed with lutetium dotatate was among the highest observed in neuroendocrine tumors to date. The safety findings were consistent with the known safety profile for 177-lutetium dotatate. No new safety concerns have emerged in this patient population.
Our study showed significant progression-free survival and unprecedented response rates, offering a new, safe treatment option in a field with no established standard of care.
“These data have practice-changing implications and support consideration of first-line use of lutetium dotatate in high-grade 2 and grade 3, well-differentiated, gastroenteropancreatic neuroendocrine tumors.” Singh S, et al: ASCO GiCS 2024; Abstract LBA588.: ASCO Post January 2024
Next Steps with NETTER-2
The NETTER-2 study will continue to collect additional safety and overall survival data for a long-term follow-up of 3 years. Patients in the study also have the option to participate in an optional crossover or re-treatment phase after experiencing disease progression, subject to meeting specific protocol criteria.
–

–
Responses to NETTER2 report:
Many initial responses to this news have been positive, but also sound a note of caution – for several reasons:
–

” … Results from NETTER-2 were published over the weekend. The study’s primary endpoint was to prove that Lutathera in combination with long-acting octreotide prolonged progression-free survival (PFS) in GEP-NET patients with well-differentiated, advanced G2 and G3 tumours. Results included meeting the primary endpoint with an extended median progression-free survival (PFS) to 22.8 months in the Lutathera and octreotide LAR arm compared to 8.5 months with high-dose octreotide LAR alone. Data analysis of secondary endpoints including overall survival and long-term safety data continues.
Importantly this study looked at using Lutathera as a first-line molecular radiotherapy with long-acting octreotide in patients with advanced neuroendocrine neoplasms. It strengthens evidence for the use of molecular radiotherapy earlier in the treatment pathway of neuroendocrine neoplasms as well as supporting use in well-differentiated G3 NENs.” Dr Amy Eccles, Consultant Radiologist at Imperial College Healthcare NHS Trust London, UK
A key question in the management of patients with GEP (and lung) NETs is the type and order of treatments – what is the ideal sequencing of 177Lu-DOTATATE in relation to other treatments?
Published consensus guidelines would suggest that SSAs are not routinely used in high-grade NETs – so questions have been raised around Octreotide as a comparator in the study. However, we should be mindful that guidelines are recommendations, some with varying levels of supporting evidence.
–
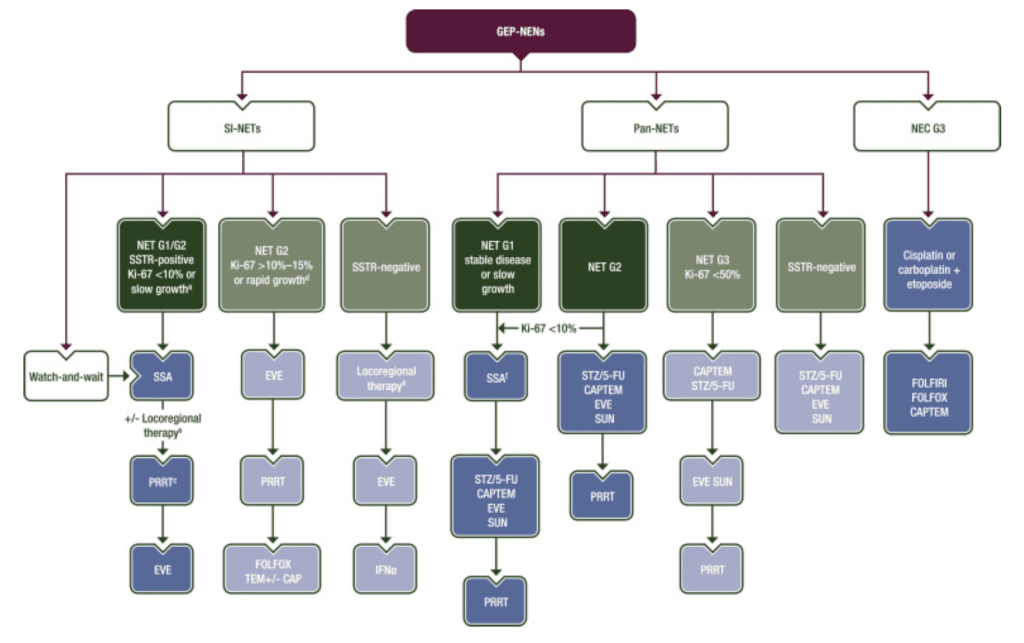
Image source: Pavel et al (2020) ESMO Clinical Practice Guideline
–
A recent review, published in the Journal of Nuclear Medicine, this month explores the sequencing question – but concludes that :
“Decisions on treatment sequencing should be individualized on the basis of disease and patient factors. Multidisciplinary tumor boards at centers of expertise, incorporating perspectives from relevant medical specialties (e.g., medical oncology, interventional radiology, surgery, and nuclear medicine), can help to optimize treatment strategies.” Stroberg et al (2024) Journal of Nuclear Medicine, lead author NETTER-1 study
For patients and their families, NETTER-2 raises both hopes and concerns
Many in the UK recall the removal of PRRT (Lutetium (177Lu) oxodotreotide) from the Cancer Drugs Fund in 2015 and the 2-and-a-half-year odyssey to NICE approval (albeit within certain restrictions and funding agreements).
- When, where, and how might this treatment be made available?
- Will my doctor know about it?
- Will there be capacity and availability?
- How will it be funded?
- What if it isn’t?
- Will it only be available through another trial?
- What if I’m not eligible?
These questions resonate across the global community – particularly where there are already geographical disparities around access – to diagnostics, to specialist care and expertise, to recommended treatment modalities and/or clinical trials:
INCA’s 2023 global challenges paper reports on the significant variability in the availability of 68 Ga-DOTA positron emission tomography (PET)/computed tomography (CT) and peptide receptor radionuclide therapy (PRRT) across countries and continents. It also highlights a further issue regarding clinical trial accessibility, awareness, and enrolment: Only 17% (403/2359) of patients had participated in NET trials, despite 67% wanting to take part (if eligible), with nearly 80% wanting more information.
National care pathways, enhancing HCP NET knowledge, and “ensuring effective diagnostics and access to appropriate treatments are crucial to improving patient survival and NET care worldwide.” Dureja et al (2023) Journal of Neuroendocrinology: Vol 35: Issue 6
“For practitioners who are treating patients with NETs, I would strongly encourage the consideration of clinical trials that might be suitable for your patients. I know that it is not always feasible, but the only way that we can continue to move this field forward is to encourage even greater participation in the clinical trial process.” Thorvadur R. Halfdanarson, Medical Oncologist. Professor of Oncology, Mayo Clinic, USA\
NETTER-2 is good news – offering hope and potential options for treatment for those with high-grade NETs, however, real-world application and implementation issues are to be kept in mind: availability, accessibility, and affordability. Alongside keeping what matters most to those who may undergo this therapy at the forefront – do end points meet patients’ preferred outcomes?
One of the first studies to evaluate the treatment goals and preferences of adult patients with NETs – highlights this point. It found that participants valued maintaining independence and cognition (“my thinking ability” over survival (67% and 85% respectively). In terms of treatment-related impacts, 93% strongly agreed they would tolerate side effects now – “if it means I could have a better quality of life in the future”. Overall survival – regardless of quality of life – was important to about a third.
Only half believed they had the same primary treatment goal (end-point) as their physician. Li et al (2022) JNCCN: Vol 20: Issue 12
–
“Whilst we are all delighted at the positive results of NETTER-2 and PRRT / RLT as a first line treatment option for Neuroendocrine Cancer patients, consideration must also be given to those excluded from the original criteria by primary site (like myself, as a Lung NET patient). With marvellous support from my team at The Christie NHS Foundation Trust Manchester, I accessed a non-standard PRRT protocol of just 3 cycles during 2019, and have so far had 4 years of stability, despite a heavy burden of disease. I’d call that a result. We must also compare like with like, NETTER-1 was more low grade.
As a patient, my hope is to see a trial across all primary sites and with endpoints that match patient expectations on QoL at the time of treatment.” Kate Quirk, Patient Ambassador, Peer Support Lead, and Support Service Co-ordinator, Neuroendocrine Cancer UK.
 “Whilst we are all delighted at the positive results of NETTER-2 and PRRT / RLT as a first line treatment option for Neuroendocrine Cancer patients, consideration must also be given to those excluded from the original criteria by primary site (like myself, as a Lung NET patient). With marvellous support from my team at The Christie NHS Foundation Trust Manchester, I accessed a non-standard PRRT protocol of just 3 cycles during 2019, and have so far had 4 years of stability, despite a heavy burden of disease. I’d call that a result. We must also compare like with like, NETTER-1 was more low grade.
“Whilst we are all delighted at the positive results of NETTER-2 and PRRT / RLT as a first line treatment option for Neuroendocrine Cancer patients, consideration must also be given to those excluded from the original criteria by primary site (like myself, as a Lung NET patient). With marvellous support from my team at The Christie NHS Foundation Trust Manchester, I accessed a non-standard PRRT protocol of just 3 cycles during 2019, and have so far had 4 years of stability, despite a heavy burden of disease. I’d call that a result. We must also compare like with like, NETTER-1 was more low grade.Read Kate’s experience with Neuroendocrine Cancer and Treatment here.
–

–
Further information and resources:
Neuroendocrine Cancer UK community member stories:
- https://www.neuroendocrinecancer.org.uk/inspiring-patient-blog-sharing-experiences-and-finding-positivity-in-neuroendocrine-cancer-journey/ – shared June 2023
- https://www.neuroendocrinecancer.org.uk/from-cancer-diagnosis-to-parenting-with-purpose-by-kate/ – shared July 2023
- Katy’s story – shared December 2023 Newsletter: https://online.flippingbook.com/view/694996220/
Our web guide on Radiation-based therapies can be found here.
Available to view on our YouTube channel:
- Amy Eccles talk at the Neuroendocrine Cancer UK Virtual Summit 2020: here
- Radioligand Therapy (PRRT) – The Patients’ Experience (recorded 2023): here
- Dr Prakash Manoharan talk for the Neuroendocrine Cancer UK 2023 Virtual Conference: here
Addressing Radioligand Therapy Issues:
In the UK, and as part of an International Expert Advisory Group, Neuroendocrine Cancer UK was a key partner and stakeholder contributing to the Health Policy Partnership “Radioligand Therapy Readiness Assessment Framework”: launched on 9 June 2021. The adapted framework for the UK was launched 3 months later, along with a situation analysis and policy blueprint based on the findings from the UK assessment.
Advocacy work continues via the BNMS MRT Consortium*: a collaboration of Nuclear Medicine (and aligned) clinicians, scientists, technicians, nurses, researchers, advocates, policymakers, and patient representatives.
(The BNMS MRT Consortium* is the British Nuclear Medicine Society Molecular Radiation Therapy group)
Radionuclides for Health UK: advocate for the establishment of a stable UK supply of radionuclides for health and medical use, working with the National Nuclear Laboratory and organisations such as the BNMS (British Nuclear Medicine Society). Their published White Paper can be found here.